
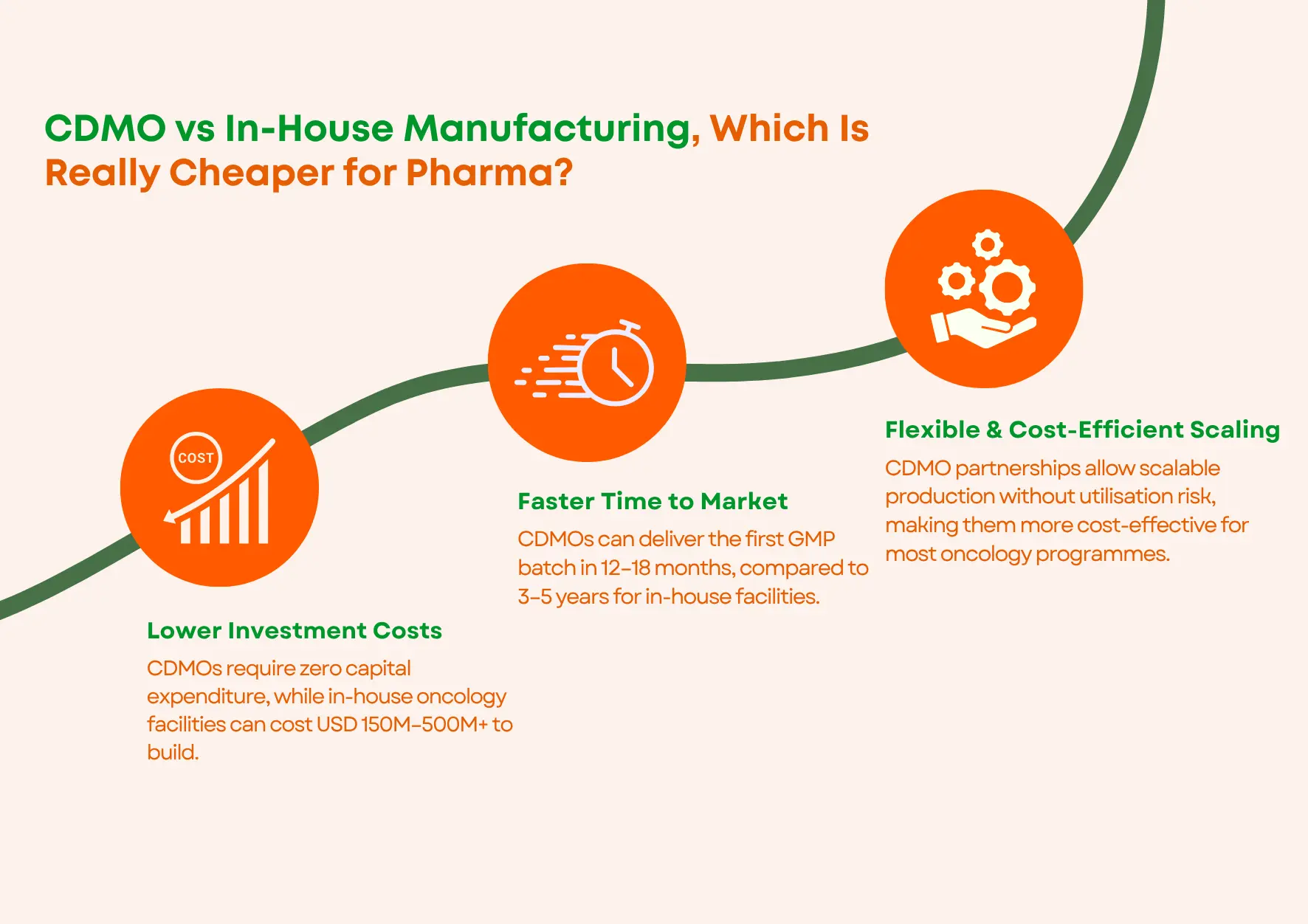
For most pharma companies, a CDMO partnership is significantly cheaper than building in-house. An in-house oncology manufacturing facility costs USD 150M–500M+ to build, takes 3–5 years to reach the first commercial batch, and carries full utilisation risk on your balance sheet. A CDMO requires zero capital expenditure, delivers your first GMP batch in 12–18 months, and lets you scale volume up or down by contract. When every cost is counted honestly, not just the building, the total cost of ownership almost always favours the CDMO model for oncology programmes below USD 400–500M in annual revenue.
Here is a question that keeps pharma CFOs up at night.
Do we build our own oncology manufacturing facility, own the asset, control the process, cut out the third-party margin? Or do we partner with a specialist oncology CDMO and stay lean, fast, and focused on what we actually do best?
On paper, in-house looks like the smart long-term play. In reality, when you add up every cost, not just the building, but everything the building brings with it, the picture looks very, very different.
This guide gives pharma CFOs, finance directors, VP Operations leaders, and commercial teams an honest, complete framework for making the make-versus-buy manufacturing decision in 2026. Real numbers. Plain language. No spin in either direction.
First, What Does “Total Cost of Ownership” Actually Mean in Pharma?
Most financial comparisons between in-house and CDMO manufacturing focus on one number: capital expenditure. The cost to build the facility. And on that single metric, in-house often looks competitive.
But total cost of ownership (TCO) means something different. It means: what does this decision actually cost over the full commercial life of the product, every rupee, every dollar, including the ones that never show up in the initial business case?
In pharma manufacturing, honest TCO includes:
- The capital cost to build and fully validate the facility
- The ongoing annual cost of GMP compliance and regulatory readiness
- The full-time staff costs, scientists, QA managers, engineers, on your payroll permanently
- The commercial revenue lost during the 3–5 years you are building and waiting for regulatory approval
- The cost of unused manufacturing space when product volumes miss projections
- The opportunity cost of capital that cannot go into your pipeline, your licensing deals, or your market expansion
When all of these are on the table, the CDMO partnership model almost always delivers better economics, especially for oncology, where containment infrastructure, regulatory complexity, and technical demands are the highest in the industry.
Let us break this down properly.
The Real, Full Cost of Building Your Own Pharma Manufacturing Plant
The 6 Hidden Costs That Never Appear in the Initial Business Case
Most finance teams put one number in their in-house manufacturing business case: the facility build cost. Here are the six costs that get left out, and should not be.
Hidden Cost 1, The Building Is Just the Beginning
A GMP-certified oncology manufacturing facility costs between USD 150 million and USD 500 million to build, fit out, and fully validate, before a single commercial batch is produced. And that is under ideal conditions. Cost overruns of 20–30% are common in pharmaceutical construction. The figure on your business case is almost always a floor, not a ceiling.
Add to that: a dedicated OEB Level-5 containment suite for cytotoxic oncology APIs costs an additional USD 30–80 million per certified suite. If your pipeline includes HPAPIs, and most modern oncology pipelines do, that cost is not optional.
Hidden Cost 2, Regulatory Approval Takes Years After Construction Ends
Here is the part that catches most teams off guard. After the building is complete, after every piece of equipment is installed, every system validated, every document written, you still need FDA, MHRA, and EU-GMP inspections before you can release a single commercial batch.
Getting through all three regulatory approvals for a brand new facility typically takes 24 to 36 months post-construction. That is two to three years of facility running costs, loan repayments, and staff salaries, with zero revenue coming in.
A CDMO partner with existing USFDA, MHRA, EU-GMP, and ANVISA approvals is ready on day one. You skip this entirely.
Hidden Cost 3, You Need a Full Expert Team. Forever.
An oncology manufacturing facility does not run itself. You need GMP-trained pharmaceutical scientists, formulation specialists, analytical chemists, quality assurance managers, regulatory affairs professionals, production operators, and maintenance engineers, all on your permanent payroll.
A facility of meaningful oncology manufacturing capacity needs 150 to 300 full-time employees at minimum. These costs do not fall when your product has a slow quarter, when a clinical trial is delayed, or when the market shifts. They are fixed. Every month. Every year. For the life of the facility.
A CDMO partnership requires zero permanent headcount additions from you. Their team is part of the service.
Hidden Cost 4, Your Capital Is Locked in Bricks and Machines
Every rupee or dollar invested in a manufacturing building is a rupee or dollar that is not available for R&D pipeline investment, licensing deals, geographic market expansion, or business development.
For most pharmaceutical companies, the real competitive advantage is in drug discovery, clinical development, and commercial execution, not in manufacturing assets. Locking hundreds of millions into a building may feel like strategic strength. In most cases, it is a strategic misallocation of capital that constrains your options for years.
The pharma asset-light model, partnering with a specialist CDMO and deploying capital into your core strengths, consistently outperforms the vertically integrated model for companies below blockbuster-product scale.
Hidden Cost 5, What Happens When Volumes Miss Projections?
A facility built to manufacture a product at peak volume projections becomes a stranded cost the moment those projections are not met. Products underperform their commercial forecasts. Clinical pipeline molecules fail in late-stage trials. Competitors launch earlier than expected. Patents expire ahead of schedule.
At 60% utilisation instead of the 85% your business case assumed, your per-unit manufacturing cost rises sharply, and there is no easy lever to pull to reduce the fixed cost base. The building costs what it costs, regardless of how many tablets come out of it.
With a CDMO partnership, volume risk is shared across the CDMO’s full client base. Their facility utilisation is not your problem to carry.
Hidden Cost 6, Technology Moves On. So Does the Investment Required.
Pharmaceutical manufacturing technology is not static. Continuous manufacturing, real-time release testing, advanced process analytical technology, these are becoming standard GMP expectations, not optional upgrades. An in-house facility built today will need a significant technology refresh in 8–10 years to remain compliant and competitive.
CDMOs invest continuously in upgrading their infrastructure across their entire client base. When a specialist oncology CDMO upgrades its isolator systems, analytical platforms, or manufacturing controls, every client programme on that platform benefits, without carrying the capital cost of the upgrade individually.
The Real Cost of a CDMO Partnership, And Why Per-Unit Comparisons Mislead
The 3 Reasons the Standard “Per-Unit Cost” Comparison Is Wrong
The most common objection from finance teams sounds like this: “Our internal model shows we can manufacture this tablet at X per unit. The CDMO is quoting 1.4X. That is 40% more expensive. We should build in-house.”
This comparison has three fundamental errors built into it.
Error 1, The internal model assumes perfect utilisation that rarely happens.
That internal per-unit cost calculation amortises capital expenditure over an assumed 80–85% facility utilisation rate. In practice, very few oncology manufacturing facilities sustain that utilisation consistently over a commercial product’s full lifecycle. At 65% utilisation, which is common for facilities serving a concentrated portfolio, the real per-unit cost is dramatically higher than the model shows.
The CDMO’s quoted price does not change when your product volumes fluctuate. Your in-house cost per unit does, and it rises fast when capacity goes unused.
Error 2, The internal model excludes the capabilities you would have to build separately.
When a specialist oncology CDMO quotes you a manufacturing price, that price includes access to:
- OEB Level-5 containment infrastructure worth USD 30–80M per suite
- Validated analytical methods and laboratory infrastructure
- A quality management system that has already passed FDA inspection
- An experienced oncology programme management team
- Multi-market regulatory approvals, USFDA, MHRA, EU-GMP, ANVISA
Replicating each of those capabilities from scratch, in-house, costs tens of millions of dollars beyond the facility build, and years beyond the construction timeline.
→ See everything included in Pinnacle Life Science’s oncology CDMO service scope
Error 3, The internal model ignores what it costs to be wrong.
In-house manufacturing creates strategic lock-in. If you build a facility and later decide you need to switch, because your portfolio has changed, because a superior CDMO partner has emerged, or because your product has gone off-patent, you have a very expensive building to dispose of, almost certainly at a significant book loss.
A CDMO contract can be renegotiated, restructured, or wound down at a fraction of that cost. Strategic flexibility has real financial value, and in-house manufacturing eliminates it.
Side-By-Side, CDMO vs In-House Manufacturing for Oncology
| What You Are Comparing | In-House Manufacturing | CDMO Partnership |
| Capital expenditure | USD 150M–500M+ upfront | Zero, pay per batch |
| Time to first commercial batch | 3–5 years from groundbreaking | 12–18 months from partner selection |
| Regulatory readiness | 24–36 months post-construction | Already approved, use from day one |
| Staff required | 150–300+ permanent full-time employees | Zero permanent headcount from you |
| Utilisation risk | Entirely on your balance sheet | Shared across CDMO’s full client base |
| Volume flexibility | Fixed, very hard to scale up or down quickly | Adjustable by contract terms |
| OEB Level-5 containment | USD 30M–80M extra per certified suite | Included if CDMO holds certification |
| Technology upgrades | Full cost every 8–10 years | CDMO invests, you benefit automatically |
| BIOSECURE Act exposure | Not directly applicable | Must verify supply chain compliance |
| Exit cost if strategy changes | High, stranded assets at book loss | Low, contract restructure or wind-down |
When Does In-House Manufacturing Actually Make Sense?
This guide is not a blanket argument for outsourcing. There are three specific situations where building your own pharma manufacturing facility is the right strategic call.
When Your Manufacturing Process Is a Genuine Competitive Advantage
If your synthesis route, delivery technology, or formulation method is the thing that makes your product better than every competitor, and sharing that process with a CDMO creates real, unacceptable IP exposure, then internal manufacturing may be justified on strategic grounds, even at higher TCO.
When Your Product Volume Is Very Large and Very Stable
In-house manufacturing begins to deliver genuine TCO advantages over a well-structured CDMO partnership when a single product generates sustained annual revenues above approximately USD 400–500 million over a long commercial horizon, at realistic, sustained utilisation rates. Below this threshold, CDMO economics almost always win when every cost is counted honestly.
When No CDMO Has the Technical Capability You Need
For certain highly specialised drug modalities, specific cell therapies, gene therapies, some next-generation biologics, global CDMO capacity is genuinely constrained. In these categories, building internal capability may be the only way to secure reliable supply. For standard oral solid dosage oncology programmes, this situation is very rare.
Third-Party Pharma Manufacturing, The Smart Middle Ground
There is a middle option that many pharma teams overlook: third-party manufacturing.
This means partnering with an approved manufacturer specifically for commercial-scale drug production, after your formulation development is already complete. You do not need their development services. You need their certified manufacturing capacity, their regulatory approvals, and their supply chain.
For oncology programmes targeting multiple global markets, a USFDA, MHRA, EU-GMP, and ANVISA-approved third-party manufacturer in India is the most cost-efficient structure available anywhere in the world:
- Programme startup timelines up to 90% faster than building your own facility
- Workforce costs 70–80% lower than US or European manufacturing alternatives
- Infrastructure costs approximately 85% lower, with zero compromise on international quality standards
- Immediate access to OEB Level-5 containment for HPAPI oncology programmes
The BIOSECURE Act is making this even more compelling in 2026. India-based CDMOs with no China-linked supply chain exposure are now the primary beneficiaries of global oncology outsourcing demand that was previously going to Chinese manufacturers.
The Questions Your Leadership Team Should Answer Before Deciding
Before your leadership team commits to either direction, get honest answers to these questions across your cross-functional group, finance, operations, R&D, and commercial:
- Is our competitive advantage in manufacturing, or in drug discovery, clinical development, and market access?
- How much capital could we deploy more productively if it were not locked into a building for the next 20 years?
- What is the realistic utilisation forecast for an in-house facility, based on our current and projected portfolio, not our best-case projection?
- Can we absorb a 3–5 year delay to first commercial batch, and what does that cost us in peak-pricing revenue?
- What happens to the facility if our lead oncology programme underperforms, goes generic early, or fails in late-stage clinical development?
- Is our prospective CDMO partner BIOSECURE Act compliant, and can they prove it in writing?
For most pharma companies answering these questions honestly, particularly those with diversified oncology pipelines, capital deployment constraints, or aggressive commercial timelines, the CDMO model delivers superior TCO, a faster path to first commercial batch, and significantly lower strategic risk.
Frequently Asked Questions, CDMO vs In-House Manufacturing for Pharma
Q1: What is total cost of ownership (TCO) in pharma manufacturing and why does it matter?
Total cost of ownership in pharma manufacturing means the full cost of a manufacturing decision over the product’s entire commercial life, including capital expenditure, regulatory compliance operating costs, staff costs, utilisation risk, opportunity cost of capital, and time-to-market revenue losses. Per-unit comparisons without TCO systematically make in-house manufacturing appear cheaper than it really is, because they only capture the building cost, not everything the building brings with it.
Q2: How much does it cost to build a GMP pharma manufacturing facility in 2026?
A GMP-certified oncology manufacturing facility typically costs between USD 150 million and USD 500 million or more to build, fit out, and validate, before the first commercial batch. This does not include the 24–36 months of operating costs incurred while waiting for regulatory approval, nor the additional USD 30–80 million per OEB Level-5 containment suite required for HPAPI oncology programmes.
Q3: How long does it take to start commercial manufacturing with a CDMO partner?
From CDMO partner selection through technology transfer, GMP validation batches, and first approved commercial release, the typical timeline is 12 to 18 months for oral solid dosage oncology forms. This compares to 3 to 5 years for a new in-house facility from groundbreaking to first approved batch, a difference of 2–3 years of commercial revenue.
Q4: What is third-party pharma manufacturing and when is it the right model?
Third-party manufacturing means outsourcing commercial-scale drug production to an approved external manufacturer, without using their formulation development or regulatory dossier services. It is the right model when your drug’s formulation development is already complete and you need certified, high-capacity manufacturing with the regulatory approvals to supply your target markets immediately.
Q5: At what revenue level does in-house pharma manufacturing become cost-effective?
As a general benchmark, in-house manufacturing begins to deliver TCO advantages over a well-structured CDMO partnership when a single product generates sustained annual revenues above approximately USD 400–500 million over a long commercial horizon, at realistic sustained utilisation rates. Below this threshold, and for companies with diversified pipelines, CDMO economics are almost always superior when every cost is honestly counted.
Q6: Can Pinnacle Life Science handle large-scale commercial oncology manufacturing for multiple markets?
Yes. Pinnacle Life Science’s USFDA-approved facilities in Baddi, Himachal Pradesh support oncology oral solid dosage manufacturing from clinical-scale batches through 3 billion tablets per year at commercial scale. We hold MHRA, EU-GMP, and ANVISA approvals for multi-market supply, with vertically integrated API sourcing through Aarti Drugs Ltd. for full supply chain resilience. Contact our team to discuss your programme today.
Oncology Medicine Manufacturers in India: What the Numbers Don’t Tell You
India has some genuinely strong oncology medicine manufacturers, but they’re not all built the same. Here’s what actually matters when you’re trying to find a credible partner in cancer drug manufacturing.
CDMO Companies in India: What to Know Before You Partner
India’s CDMO sector is growing fast, and for good reason. But not every partner is built the same. Here’s a practical, no-jargon guide to understanding what CDMO companies in India actually offer and how to choose wisely.
CDMO Full Form: What Is a CDMO in Pharma and How Does It Actually Work?
CDMO stands for Contract Development and Manufacturing Organization. But knowing the full form is just the starting point. Here’s what CDMOs actually do, why they matter in pharma, and how they’re different from CMOs and CROs.
